Improving Breast Cancer Outcomes in Rural Appalachia – Why and How?


Abstract:
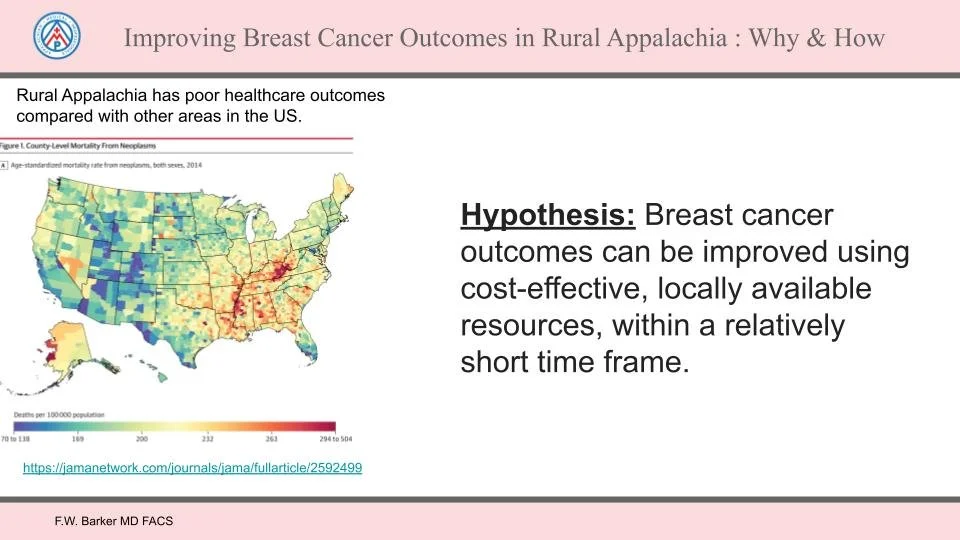
An article published in JAMA in 2016 highlighted US county to county health outcome disparities. Among them was the death rate from cancer (1). The paper reported that certain counties in rural Appalachia ranked near the very bottom. Those counties include counties in which we practice. Breast cancer is a common malignancy among women. It results in considerable morbidity and mortality. Nevertheless, substantial outcome improvement can be expected through improving breast cancer screening quality, availability and compliance, as well as by ensuring local availability of optimal, cost effective treatment options.
In the study we have initiated, historical outcomes analysis of breast cancer screening rates, screening performance, treatment interventions and costs, which will be analyzed within 15 selected rural Appalachian counties in VA and WV. Newly available artificial intelligence (AI) software for interpretation of screening mammography will be made available, www.mammoscreen.com. Baseline data will be compared with post intervention data, to determine the measure of success or failure of several relatively simple and inexpensive interventions, to improve breast cancer outcomes in rural Appalachia.
Interventions will include the development and/or local availability of:
A website for Appalachian Medical Professionals, www.wvvaamp.org, designed to
provide culturally targeted, trustworthy, science based information to area healthcare providers and their patients.
Analysis of screening compliance rates.
AI software for screening exam interpretation
A training program for breast cancer patient navigators.
Promotion of intra operative radiation therapy (IORT) for properly selected women with early stage breast cancer.
Results of the study will be compiled and reported annually, to allow comparison with other geographic areas which may have chosen similar and/or different approaches for breast cancer outcome improvement. Collaboration with and participation by local healthcare providers, breast cancer specialists, regional tertiary healthcare facilities and area breast cancer survivors will be actively encouraged.
(1) https://jamanetwork.com/journals/jama/fullarticle/2592499
Introduction:
Breast cancer is a common malignancy among American women and causes considerable mortality and morbidity. This is especially true in rural Appalachia.
However, breast cancer outcomes can be significantly improved by improving breast cancer screening, its quality, availability, and participation, as well as by boosting the local availability of affordable and effective treatment options.
An article published in the Journal of the American Medical Association (JAMA) in 2016 highlighted disparities in health outcomes in counties across the U.S. The article looked at death rates from cancer. Unfortunately, certain counties in rural Appalachia ranked near the very bottom.
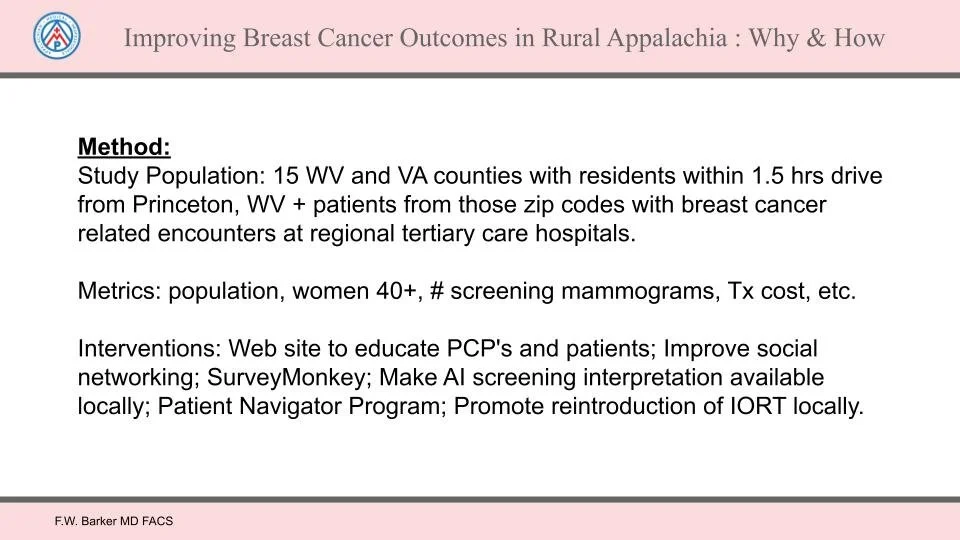
This project will analyze breast cancer screening compliance rates, introduce Artificial Intelligence (AI) software for image interpretation, treatment interventions and costs in 15 selected rural Appalachian counties in VA and WV.
It will compare baseline data with post-intervention data and try to quantify the success or failure of several relatively simple and inexpensive interventions. The overall goal is to improve breast cancer outcomes in rural Appalachia.
Method:
Interventions will include:
Developing a website for Appalachian Medical Professionals, www.wvvaamp.org, aimed at providing, trustworthy, science-based, culturally targeted, information to area healthcare providers and their patients.
Making MammoScreen, an AI software for interpretation of screening mammography, available to area mammography facilities, www.mammoscreen.com.
Assisting clinics and primary care providers to improve annual screening compliance of their women patients 40 and older.
Promoting Intraoperative Radiation Therapy (IORT) for properly selected women with early stage breast cancer.
Developing and implementing a program to train breast cancer patient navigators.
The results of the project’s analysis will be reported annually, and will provide comparison for efforts undertaken in other geographic areas. In addition, our effort will seek to foster participation and collaboration among area breast cancer specialists, healthcare providers, regional tertiary healthcare facilities and breast cancer survivors.
Breast Cancer Fundamentals:
Early detection is the bedrock of better breast cancer outcomes.
Annual Screening is key to an effective early detection program.
Innovative technologies, including 3-D mammography, breast ultrasound, contrast enhanced mammography (CEM), Artificial Intelligence (AI) image interpretation, breast MRI and Intraoperative Radiation Therapy (IORT) are important components of a comprehensive breast care program.
A network of breast care specialists, who are linked through virtual interconnectivity, reinforces the program and broadens its delivery.
Patient navigators strengthen the relationships between patients and their care teams.
Measuring Improvements:
In addition to exploring how breast cancer outcomes in rural Appalachia can be improved, it is important to examine how these improvements can be measured. What values should we look at? How can they be measured objectively? Most would agree that the most important parameter to improve is survival.
However, measuring survival is not quite as simple as it seems. Are we talking about “disease-free survival”? By this, we mean intervening, so the patient eventually has no demonstrable breast cancer, and later dies of some other unrelated cause. Or, are we measuring “overall survival”? In other words, how long did the patient survive, even after having had a recurrence of breast cancer? What about estimating the expected number of years lost to a woman’s breast cancer. This can be expressed as “Life Years Lost” (LYL). Curing breast cancer for a 42-year-old woman reduces the number of life years lost by a greater number than curing breast cancer in her 85-year-old grandmother.
What value should be placed on reducing disparities? We know that African-American women tend to develop breast cancer at a younger age,and at a higher rate than Caucasian women. As a group, they often face a more aggressive form of breast cancer as well. Another important variable is disparity based on a patient’s income.
Do poorer women suffer from less favorable outcomes than wealthier women? How should the differences in outcomes be measured?
It’s important to note that survival is not the only important factor that needs to be examined and measured. Costs should also be measured, cost to both patients and the healthcare system. Morbidities associated with treatment also deserve consideration. Cosmetic outcomes, time away from work, impact on family, may also weigh on a woman’s decision to opt for one treatment program over another.
The Rationale for choosing to study breast cancer outcome improvement
Now, let’s return to the article mentioned at the top of this paper, to better understand why we chose improving breast cancer outcomes in rural Appalachia as our initial project.
The 2016 article in JAMA entitled “US County Level Trends and Mortality Rates for Major Causes of Death,1980–2014” can be found here: JAMA Network Article The article reported cause specific mortality rates and found large differences between U.S. counties. Importantly, for every cause studied, with the exception of “mortality from neurologic disorders”, our region of rural Appalachia ranked at, or near, the very bottom.
Furthermore, “The Commonwealth Fund 2022 Scorecard on State Health System Performance” ranked West Virginia 49th out of 51 overall, 32nd out of 51 for prevention and treatment, 51st out of 51 for avoidable use and cost and healthy lives, and 43rd out of 51 for racial and ethnic equity. Clearly, we have room for improvement. The Scorecard can be found here: Commonwealth Fund
Significantly improving breast cancer outcomes can occur without major behavioral changes. For decades, the mantra has been repeated that early detection of breast cancer saves lives. As a result, screening mammography has never become the divisive issue that occurred with vaccinations, masking, and social distancing, as occurred during COVID-19. Furthermore, for decades, breast cancer specialists have understood that screening asymptomatic women for breast cancer with mammography can result in a substantial reduction in breast cancer mortality. The principal questions that remain involve the questions of when should women begin screening, and how frequently should screening take place?
If we compare treating breast cancer to treating cardiovascular disease, which was found to be the most frequent cause of death for both women and men in our region, we find that improving mortality and/or reversing contributory factors of cardiovascular disease mortality is complicated. It requires that patients commit to considerable and challenging lifestyle changes, such as smoking cessation, regular exercise, dietary changes, and reliably taking medication to better control blood pressure and blood sugar.
Importantly, positively impacting the most important factors for improving breast cancer outcomes is much simpler. Most of the elements for a program to improve breast cancer outcomes are already available in our area, or can be developed at relatively modest cost.
Therefore, it would appear that improving breast cancer outcomes in rural Appalachia is an excellent community project. We should embrace it and make it our priority. You can learn more here: VIDEO: "Screening Saves Live"
A Short History on Treating Breast Cancer:
In 1882 William Halsted performed the first radical mastectomy. The surgery required removing the breast, skin, the chest wall muscles with en bloc removal of axillary lymph nodes, this operation remained the standard operation to treat breast cancer until the mid-20th century.
In 1895, the first x-ray was taken. X-rays have evolved, such that now, low-dose mammograms are used as the principal screening technique for identifying sub-clinical breast cancer, (breast cancer that can be identified before it can be felt on a physical exam.
In 1898 the Curies discovered the radioactive elements of radium and polonium. Shortly after that, radium was used as a basis for cancer treatment.
In the mid-1930s doctors and researchers developed a new approach to mastectomy. It was called the modified radical mastectomy. It was less disfiguring, and it became the new standard of surgical treatment for breast cancer until the early 1970s.
In 1977, the Swedish Two County Trial (STCT) began. The STCT enabled doctors to better understand the impact of identifying sub-clinical breast cancer (breast cancer before it can be detected by a physical exam). The STCT ended in 1985 with reports showing that women between 40 and 79 years old, who had a single view, analog mammogram every other year, experienced about a 30% reduction in mortality compared to women who were diagnosed and treated only after their breast cancers become clinically apparent, You can learn more about this here: Swedish Two County Trial
The Food and Drug Administration (FDA) has also made major contributions to improving breast cancer outcomes. More than 40 years ago, the FDA approved Tamoxifen, an estrogen receptor modulator. Many medications for treating and preventing breast cancer have been developed since then.
In recent decades, new surgical approaches have been developed that produce less disfigurement and morbidity. They include sentinel lymph node biopsy, skin and nipple sparing mastectomy, oncoplastic surgery and a wide variety of breast reconstruction techniques. These surgical advancements all aim to improve cosmetic outcomes without sacrificing the ultimate goal of cure.
In 2018, a clinical trial suggested that chemotherapy after surgery does not benefit the vast majority of women who have early-stage breast cancer. Learn more about, Less is More. High dose chemotherapy with bone marrow transplant was also ruled out as a good treatment option. In other words, a “less is more” approach continues to play an important role in treating breast cancer.
Recently, another trial, called the TARGIT-A trial, looked at long term follow-up results of women who were enrolled in trial and found that long-term survival of lumpectomy with intraoperative radiation therapy (IORT) at the time of surgery resulted in equivalent long-term survival, in addition to other advantages, when compared with women having lumpectomy and more conventional postoperative whole breast external beam radiation. This is another example of “less is more” when it comes to treating breast cancer. You can learn more here:https://targetbreastcancer.org.
My Story as a Breast Cancer Specialist:
During my surgical training (1981-86), “breast specialists” were generally found only at major metropolitan and university cancer centers. These facilities include Memorial Sloan-Kettering Cancer Center, where I trained, MD Anderson, Roswell Park, Mayo Clinic and a number of others. Today, there is an abundance of doctors who specialize in breast cancer diagnosis and treatment practicing in a wide variety of settings.
Starting in the late 1980s, a few radiologists began experimenting with using stereotactic techniques for biopsy of non-palpable, mammographic abnormalities. You can learn more here: Stereotactic Biopsy
In 1992, I saw a Fisher stereotactic breast biopsy system for the first time at the American College of Surgeons Clinical Congress.
It was obvious to me that this would become the future of breast biopsy, given that it offered women a minimally invasive breast biopsy to detect cancer. Performing stereotactic procedures responsibly requires a familiarity with mammography. So, I began to educate myself about mammography by attending a mammography course offered by Dr. Laszlo Tabar. I also read his books.
Tabar was one of the principal investigators of the Swedish Two County Trial (STCT), perhaps the most important study demonstrating that regular mammographic screening of asymptomatic women results in a significant improvement in breast cancer mortality. Dr. Tabar’s course was the best course I have ever attended on any subject. Soon, I became a screening mammography “true-believer.”
The STCT, which began in 1977, enrolled 77,080 women, 40–74, who were invited to active screening with a single view mammogram every two years. The outcome of this group was then compared with that of a group of 55,985 women 40–74 who were given “passive breast care” by their doctors. Passive breast care means treatment initiated only after the breast cancer became clinically apparent - in other words, it became palpable. At year six, all women were invited to have a single view screening mammogram and the study was closed at year seven. In 1985, the first mortality results were published and the results showed a 31% mortality reduction in the active screening group. That improved outcome has persisted, and even increased, even after more than 30 years of follow-up.
The information found in Breast Cancer - The Art and Science of Early Detection With Mammography: Perception, Interpretation, Histopathologic Correlation, by Dean, Tabar et al. demonstrates that smaller size at detection results in longer survival.
Importantly, to achieve a 95% or better chance at survival, breast cancer must be detected before it grows larger than the average size of a breast cancer detected on a first mammogram. This is smaller than the average size of breast cancer detected by regular breast self-exam , or much smaller than the size of breast cancer detected by a woman through unplanned breast self-exam.
Therefore, it became obvious that to optimally reduce breast cancer mortality, the cancer must be detected before it grows larger than about 14 mm. It’s also important to detect breast cancer in a cost-effective fashion.
Since 1977, when the STCT began, there have been significant improvements in breast imaging technology. For starters, four-view screening mammograms have been found to be superior to single view screening mammograms, which was used in the STCT.
Analog film screening mammograms, like those used in the STCT, are no longer used in the U.S. They have been replaced, first by digital mammography, and more recently by Digital Breast Tomography (DBT). This more recent technology has been found to be up to 40% more accurate.
Furthermore, many breast imaging experts support annual screening regimens, rather than biannual exams, especially for younger women, and those at higher risk.
Improvements in breast ultrasound, breast MRI and recently contrast enhanced DBT have also been shown to be useful in appropriate settings.
Learn more here: VIDEO: Contrast-Enhanced Mammography
In today’s world, “report cards of quality breast care,” including guidelines for interpreting screening mammograms, exist. Women and their primary care physicians should ask mammography facilities about the cost and quality of the screening mammography they offer. This is because different facilities have different contracts with payors, so the costs may differ, despite being identical services. Metrics of quality are tracked and reported annually by all certified facilities.
My White Papers
During my 3 decades of surgical practice, I have written several white papers about breast cancer care in our local area. The first one was entitled, “Center for Breast Health 1993-1994.”
In addition to stating the obvious, that early detection of breast cancer is the key to improving survival and that high-quality mammography is the cornerstone of early detection, I went on to state that, “It is well recognized by breast cancer experts that women are optimally served in the management of breast cancer through multidisciplinary breast centers; centers which coordinate all aspects of care from education and imaging through treatment, counseling and follow-up.” I continued that, however, “there is ... a significant segment of the rural population which is unlikely to venture independently to this type of center. Therefore, a combination of a centrally coordinated program with outreach capabilities for imaging, education and physical exam represents the best possibility for providing optimal care for all women throughout ... [our] service area.”
In describing my thoughts on what an optimal initiative for improving breast cancer outcomes in rural Appalachia might look like, I went on to say, “high-quality breast imaging is the corner-stone of a multidisciplinary breast cancer center. In addition, a dependably high-volume and streamlined, efficient operation are key to such a program’s survival. Factors that warrant consideration in designing a program include the following:
Distinction between screening and diagnostic mammography.
Selection of a site that will: meet the needs of the community while providing consistent, high volume.
Low examination cost for screening mammography coupled with detailed financial analysis and reappraisal on an ongoing basis.
A customized marketing program that incorporates methods to increase awareness, compliance, and utilization by women and referring physicians.
A well-trained, efficient, and dedicated staff.
An operation that is designed for rapid and efficient patient flow.
A plan for streamlined image handling, interpretation, reporting and storage.
Timely communication of examination results to referring doctors and patients.
Effective follow-up and analysis of outcome data.
Establishment of a consistent and reliable quality assurance program to monitor all aspects of the center’s services.
Conclusion:
It’s noteworthy how little the basics of treating breast cancer have changed since writing that white paper. The mission for such a breast cancer center has several important dimensions. First, to provide optimal coordination of an early detection program -– screening. Second, to provide multidisciplinary coordination of care of women in the region, after they have been diagnosed with breast cancer.
Ultimately, success will depend on a well-coordinated effort of all regional stakeholders and a willingness of our community to support a change of the status quo.
Creating a not-for-profit facility would be helpful, due to its ability to apply for grant funding and provide non-competitive coordination of services. Actually, such an initiative is already possible. The West Virginia based Community Connections Inc. www.strongcommunities.org, is a charitable not-for-profit. Its partner, Appalachian Medical Professionals Inc. www.wvvaamp.org is also a not-for-profit organization and it is ideally suited to the task of organizing physicians, nurse practitioners, and patient navigators.
For the development of a locally-based, virtual multi-specialty breast center, “patient navigators” are key. These navigators can make sure that the highest possible number of area women are successfully screened for breast cancer. Once women are diagnosed with breast cancer, the patient navigators can also help coordinate the patient’s care.
This approach has already shown improved breast cancer outcomes in Delaware. CMS grants are currently available to pay for patient navigators, and the Biden administration has made “The Cancer Moonshot”, reducing cancer mortality by 50% over the next 25 years, one of its priorities. https://www.whitehouse.gov/cancermoonshot/
We already have most of the elements necessary for improving breast cancer outcomes in rural Appalachia. What we really need, is to better educate ourselves about currently available resources, and then coordinate and secure the most important ones. To that end I have prepared a short list of reliable resources.
I also hope we will soon make IORT for early stage breast cancer available locally again. It has been available at WVUMedicine in Morgantown, W.V. since 2015.
It is an unfortunate fact that few women in our area are willing, or able, to travel that far to receive this important treatment innovation. VIDEO: IORT for Breast Cancer
The TARGIT-A Trial, a 20-year IORT outcome results report can be found in this article: TARGIT-A Results. If properly selected, survival with lumpectomy and IORT is equivalent to standard breast conservation approach with whole breast external beam radiotherapy, but it has numerous important advantages to the patient. VIDEO: IORT
Unfortunately, recent guidelines for radiation for early stage breast cancer proposed by the American Society for Therapeutic Radiology and Oncology, (ASTRO), currently discourage the use of IORT for the treatment of early stage breast cancer outside the realm of a formal clinical trial. In my opinion, this is one more case in US healthcare, where financial interests of privileged stakeholders trump the best interest of individual patients.
Final Recap:
Early detection is the bedrock of better breast cancer outcomes.
Annual Screening is key to an effective early detection program.
Innovative technologies, including 3-D mammography, contrast enhanced mammography (CEM), breast ultrasound, Artificial Intelligence (AI) image interpretation, breast MRI and Intraoperative Radiation Therapy (IORT) are important components of a comprehensive breast care program.
A network of breast care specialists who are linked through virtual interconnectivity can strengthen the program and broaden its delivery.
Patient navigators strengthen the connection between patients and their care teams.
Additional Resources:
Contrast-Enhanced Mammography: Current Applications andFuture Directions
https://pubs.rsna.org/doi/full/10.1148/rg.2019190079
Digital Breast Tomosynthesis: Concepts and Clinical Practice
https://pubs.rsna.org/doi/full/10.1148/radiol.2019180760
State of the art of minimally invasive breast biopsy: Principles and Practice
https://link.springer.com/article/10.1007/BF02966407
Breast cancer screening guidelines
https://www.jacr.org/article/S1546-1440(21)00383-5/fulltext?_ga=2.147172727.118277 6748.1648219869-1456358389.1647718250
IntraOperative Radiation Therapy for Breast Cancer (IORT)
https://www.youtube.com/watch?v=_VsRASUrWrY
Breast Patient Navigators
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4121958/
NCCN Patient Information
https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1419
Patient information from UpToDate
https://www.uptodate.com/contents/table-of-contents/patient-education